126
Views & Citations10
Likes & Shares
Materials and Methods: a quantitative study conducted at the Intensive Care Unit (ICU) of Semen Gresik Hospital. The research design used was the post-test only control group design experimental approach. The sampling method used was purposive sampling. The sampling taken were 16 respondents. The independent variable is the act of using a sponge belt restraint strap modification. The dependent variable is injuries in patients with decreased consciousness. Data retrieved using observation. Data were analyzed by Wilcoxon Test analysis. Adjusted odds ratio (ORs) with 95% confidence interval (CI) was calculated.
MATERIALS AND METHODS
The research used experimental research with design study was the Post-test Only Control Group Design Experiment. The independent variable in this study was the use of a sponge belt restraint strap modification and the dependent variable was injury in patients with decreased consciousness. Sample in this study used a sample of 16 respondents with a purposive sampling technique. The procedures and respondents involved in this research were appropriate of Ethical Clearance (EC) with No.038/UG. R/ET/2020. Data retrieved using observation /checklist for standard operational patient safety with restrains. Data were analyzed by Wilcoxon Test analysis. Adjusted odds ratio (ORs) with 95% confidence interval (CI) was calculated.
RESULTS
Of the 16 patient respondents who met the requirements as respondents, the following characteristics were obtained:
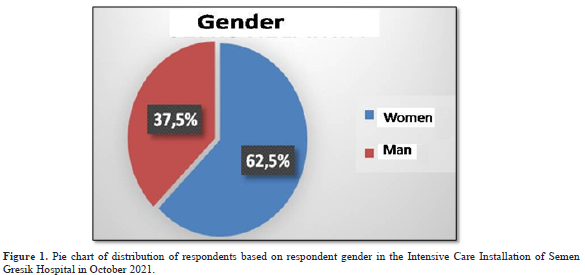
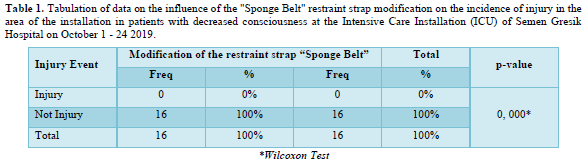
- Characteristics of Respondents Based on Gender
Figure 1 shows that the distribution of respondents based on gender was mostly women, 10 people (62.5%).
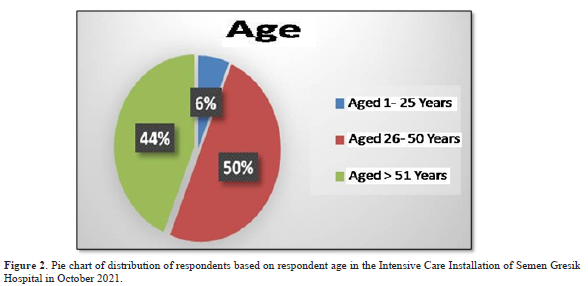
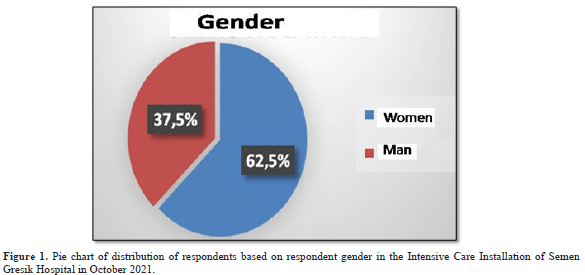
- Characteristics of Respondents Based on Age
Figure 2 shows that the majority of respondents are aged 26-50 years as many as 8 people (50%) and a small portion are aged 1-25 years as many as 1 person (6.25%).
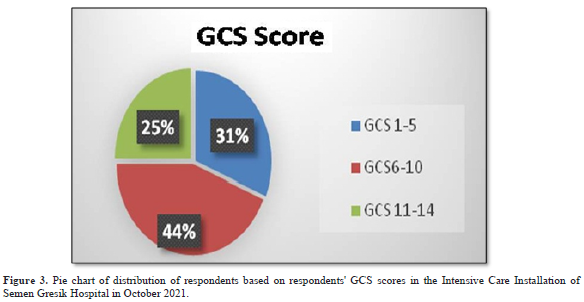
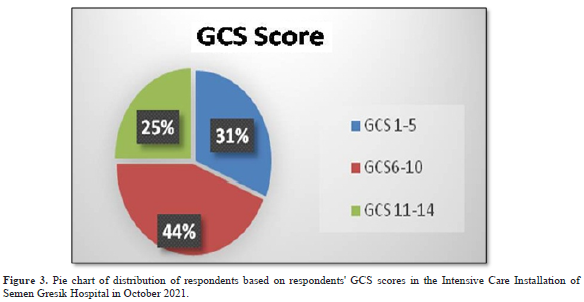
- Characteristics of Respondents Based on GCS Scores
Figure 3 shows that the majority of respondents had a GCS score of 6-10 as many as 7 people (43.75%) and a small percentage of respondents had a GCS score of 11-14 as many as 4 people (25%).
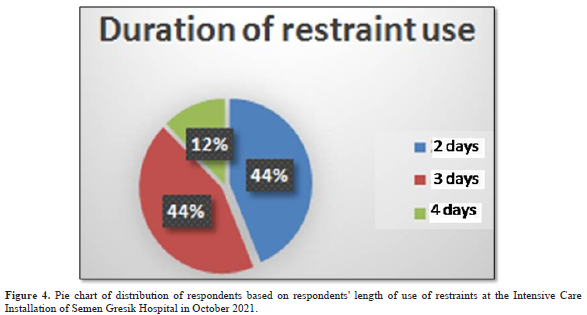
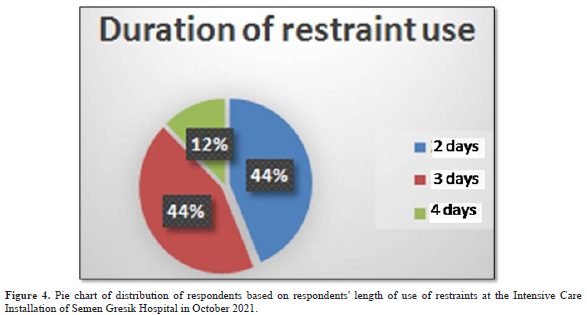
- Characteristics of Respondents Based on Length of Restraint Use
Figure 4 shows that the majority of respondents had a duration of restraint use of 2 and 3 days, namely 7 people each (43.75%) and a small number of respondents had a duration of restraint use of 4 days, namely 2 people (12.5%).
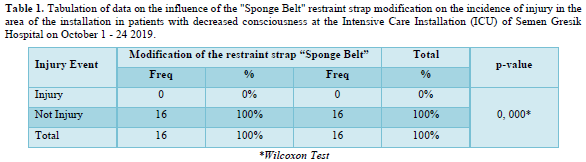
The influence of the "Sponge Belt" restraint strap modification on the incidence of injury in the area of the installation in patients with decreased consciousness are shown in Table 1. that none of the respondents suffered injuries, as many as 16 respondents (100%). The analysis showed that the significance level p = 0,000 means that there was a significant influence on the incidence of injury in the installation area after the rope modification “Sponge Belt" restraint is α <0.05 (Table 1).
DISCUSSION
The research results showed that the most common characteristics of patients in the gender group were women (62.5%) while the number of patients was men (37.5%). The results of this study do not match the results of research conducted by Wanda (2003) which stated that the number of male patients was greater than female patients. The results of the research show that the ages of respondents in the general tabulation data are mostly 26 - 50 years old, 8 people (50%), this is in accordance with the theory of Videbeck (2008), which states that the highest incidence of injuries due to binding treatment is in the range aged 25-45 years. Where this productive age has the strength to fight back when restraint is carried out so that it can result in injury. However, after using the modification of the "Sponge Belt" restraint strap on patients with decreased consciousness, no injuries occurred because the material used in making the restraint used a sponge base so it was comfortable to wear and used silica drill cloth which can absorb sweat. The GCS scores for most patients were 6-10, as many as 7 people (44%), where the GCS score was the middle level of consciousness [15]. This can affect the patient's movement, possibly causing abrasions on the skin of the extremities. However, we use a modification of the "Sponge Belt" restraint strap which has a strap with two sides and a length of 50 cm to facilitate the tying process and has double fixation, namely using a belt and adhesive. So that no injury occurs due to patient movement. Based on the research results, it shows that most of the duration of restraint use is 2 and 3 days, namely 7 people each (44%). A safe duration based on literature sources, both according to CMS Psychiatric Residential Treatment Facilities, COA, and JCAHO, the period of restraint action for mental disorders patients over 18 years of age is more than 4 h. This is done to minimize the side effects of the restraint procedure, but basically there is no standard for a good length of binding. Each institution or department that handles the preparation of SOPs has different policies in determining the duration of this engagement. However, other literature adds, as stated by the Idaho Department of Correction (2010) in the SOP for restraint measures, the maximum initial duration of restraint intervention is 8 h. After the 8 h period has ended, a re-evaluation is carried out regarding the patient's aggressive behavior. If the behavior displayed by the patient is still the same and has not shown improvement, then the restraint procedure can be applied again if other alternative steps to control behavior have not been effective. However, the use of modified "Sponge Belt" restraint straps in patients with decreased consciousness does not result in injury, this could be because the material used in making the restraint uses a sponge base material so it is comfortable to wear and uses silica drill cloth which can absorb sweat, in addition to having rope with two sides and a length of 50 cm to facilitate the fastening process and has double fixation, namely using a belt and adhesive. So that no injury occurs due to patient movement during gradual observation up to a limit of 2 x 24 h. Based on data from medical records at Semen Gresik Hospital in 2018, the number of patient safety incidents before the use of modified restraint straps was carried out, the incidence of injury in the form of abrasions on the wrist was 3 incidents (50%) out of 6 KTD. This is partly due to friction between the restraint materials and the length of time the restraint rope is used. The results of a significant influence on the incidence of injury in the installation area after the rope modification “Sponge Belt" restraint. The use of modified sponge belt restraint straps in patients with decreased awareness provides a sense of security and comfort so as to avoid the occurrence of KTD. Restraint extremity is limiting the motion of extremities by using cuffs on the wrists or ankles and fastening cloth. Restraint must be done in special conditions; this is the last intervention if the client's behavior cannot be overcome or controlled with behavioral strategies or environmental modification [13]. Restraints are used when other, less restrictive interventions have been unsuccessful/ineffective in protecting the patient, staff, or others from a threat [14]. Restraint sponge belt is the name of a modified restraint for patients with decreased consciousness. The modification characteristics of sponge belt restraint straps are sponge-based belt pads, silica drill fabric that absorbs sweat, double-sided and 50 cm long ropes, simplifying the process of double binding and fixation using belts and adhesives. The results showed that the age of respondents in the general tabulation data was that most of the ages 26 - 50 years were 8 people (50%). The highest incidence of injuries resulting from the treatment of binding actions was in the range age 25-45 years. Where this productive age has the strength to fight when a restraint is taken so that it can result in injury [14]. However, after the use of a "Sponge Belt" restraint strap modification in patients with decreased awareness, injuries do not occur because the material used in making the restraint uses a sponge base material so that it is comfortable to wear and wear a silica drill cloth that can absorb sweat. Besides that, in general data tabulation the GCS value of patients is mostly 6-10 as many as 7 people (44%), where the GCS value is a mid-level awareness level [15]. The Glasgow Coma Scale has become an integral part of clinical practice and research worldwide. Findings using the scale have shown strong associations with those obtained by use of other early indices of severity and outcome [15]. This can affect the movement of the patient which allows blisters on the extremities of the skin. However, the use of a modified "Sponge Belt" restraint strap which has a rope with two sides and a length of 50 cm, facilitates the binding process and has double fixation using a belt and adhesive. So that injuries do not occur due to patient movement. Based on the results of research shows that most of the use of restraint 2 and 3 days is 7 people (44%) each. Safe duration based on literature sources, according to the CMS Psychiatric Residential Treatment Facilities, COA, and JCAHO, the duration of restraint action in patients with mental disorders aged over 18 years is a tick may take more than 4 h. This is done to minimize the side effects of the restraint procedure, but basically there is no standard long-time good binding. Each institution or department that handles the preparation of SOP has a different policy in determining the duration of this engagement. However, other literature adds, as revealed by the Idaho Department of Correction (2010) in the SOP of restraint measures, the maximum initial duration of restraint intervention is 8 h. After the 8 h period is over, a re-evaluation is made regarding the patient's aggressive behavior, if the behavior displayed by the patient is still the same and has not shown improvement, then the restraint procedure can be reapplied if other alternative measures for controlling the behavior of the results have not been effective [16]. However, the use of a "Sponge Belt" restraint strap modification in patients with decreased awareness of injury does not occur, this could be due to the material used in making the restraint using a sponge base material so that it is comfortable to wear and use a silica drill cloth that can absorb sweat, in addition to having a rope with two sides and a length of 50 cm, facilitates the binding process and has a double fixation using a belt and adhesive. So that injuries do not occur due to the movement of the patient during the gradual observation to the limit of 2 x 24 h. The impact experienced by patients during the restraint besides physical condition is also psychological. This study shows that the physical effects experienced directly in the implementation of a restraint are the emergence of physical discomfort, abrasions in the area of the restraint installation, increased risk of contractures and bone damage. The results of this study are not in accordance with the research of Kandar and Pambudi (2013) where the results of the restraint action did not cause injury so that it proved effective in reducing violent behavior [17]. However, the results of this study are consistent with the results of research conducted by Wanda [18], stating that restraint measures taken in mental patients can cause emotional trauma or psychological effects [18]. Limitations in this research are: 1) Observations are carried out only on patients who experience decreased consciousness, and sampling was only carried out on intensive care unit (ICU) patients, so the results cannot represent all patients with decreased consciousness at Semen Gresik Hospital. This study provides recommendations about modification of the Sponge belt restraint strap has the characteristics of a sponge-based belt, because it uses a silica drill that can absorb sweat, a rope with two sides and a length of 50 cm, simplifying the process of binding and double fixation, which uses a belt and adhesive. The hospital always monitors the use of restraint in patients, especially observations during restraint installation.
CONCLUSIONThe research results show no respondent experienced an injury event after using a modification of the "sponge belt" restraint strap in the mounting area in patients with decreased consciousness, and no injuries after the use of a modified "sponge belt" restraint strap in the area of restraint installation in patients with decreased consciousness. However, a significant influence of the use of a "sponge belt" restraint strap modification on the incidence of injury in the area of attachment in patients with decreased consciousness. It is hoped that nurses will always pay attention to patient safety procedures, especially in carrying out restraint actions which aim to prevent patient safety incidents from occurring by participating in training and socialization regarding restraint action techniques so that nurses can have continued professionalism in carrying out restraint actions. Hospitals always monitor the quality of patient safety by making regulations/SOPs for restraint actions on patients, especially observing the length of time the restraint strap is used.
- Health TIM (2011) Regulation of the Minister of Health of the Republic of Indonesia Number. 11 / MENKES / PER / VIII / 2017 About Patient Safety in Hospitals. pp: 41.
- Haimowits U& H (2006) Restraint and Seclusion - A Risk Management Guide.
- Ministry of Health, RI (2008) National Guidelines for Hospital Patient Safety (Patient Safety). KKP-RS Edi.
- Hospital SG (2018) Quality of Semen Gresik Hospital.
- Springer G (2015) When and how to use restraints. Am Nurse Today 10: 1.
- Videbeck L, Sheila (2008) Psychology Nursing Textbook. Jakarta: EGC.
- Kandar, Pambudi, Prabawati S (2013) Efektivitas tindakan restrain pada pasien perilaku kekerasan yang menjalani perawatan di unit pelayanan intensif psikiatri (UPIP) RSJ Daerah Dr. Amino Gondohutomo Semarang 2013 [The effectiveness of restraint on patients with violent behavior who undergo. In: prosiding konferensi nasional II PPNI Jawa Tengah 2014.
- Saseno, Pramono, Giri, Kriswoyo (2013) Pengaruh tindakan restrain fisik dengan manset terhadap penurunan perilaku kekerasan pada pasien skizofrenia di ruang rawat intensif bima Rumah Sakit Jiwa Grhasia Daerah Istimewa Yogyakarta [the effect of physical restraint with cuff on increasing violent. Jurnal Keperawatan Mersi 4(2): 1-6.
- Bryant AR, Nix PD (2007) Acute & Chronic Wounds: Current Management Concepts. Third Edit. St. Louis, Missouri.: Mosby.
- Potter PA, Perry AG (2005) Fundamental of Nursing. 4th Jakarta: Salemba Medika.
- Stubbs B (2009) The manual handling of the aggressive patient: A review of the risk of injury to nurses. J Psy Ment Health Nurs 16: 395-400.
- Happell B, Harrow A (2010) Nurses’ attitudes to the use of seclusion: A review of the literature. Int J Ment Health Nurs 19: 162-168.
- Riyadi S, Purwanto T (2009) Mental Nursing. Yogyakarta: Graha Science.
- Videbeck L, Sheila (2008) Psychology Nursing Textbook. Jakarta: EGC.
- Harsono (1996) Clinical Neurology Textbook. Yogyakarta.
- Idaho Department of Correction Law Insider (2023) Available online at: https://www.lawinsider.com/contracts/22iVltA8biB
- Kandar, Pambudi, Prabawati S (2014) Effectiveness of restraint measures in violent behavior patients undergoing treatment at the psychiatric intensive care unit (UPIP) of the Regional General Hospital, dr. Amino Gondohutomo Semarang (Efektivitas tindakan restrain pada pasien perilaku keker. In: Prosiding Konferensi Nasional Ii Ppni Jawa Tengah 2014.
- Wanda K (2003) Breakaway and physical restraint techniques in acute psychiatric nursing. J Forens Psychiatry Psychol 16: 380-398.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Advance Research on Alzheimers and Parkinsons Disease
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)


